

- Home
- Companies
- advanceCOR GmbH
- Products
- advanceCOR Revacept - Model GPVI-Fc - ...



advanceCOR Revacept - Model GPVI-Fc -Synthetic Protein
This is the name of our therapeutic agent for the prevention of stroke and heart attack. Its principle effectiveness has already been proven in patients. It is a soluble protein which, when blood vessels are damaged, covers the damaged areas. Revacept is designed to protect the vessel walls so that vascular occlusion does not occur. Revacept has been shown to be well tolerated and effective in a Phase II study in carotid artery damage and heart damage. Further studies are in preparation and modified Revacept products are in pre-clinical research.
- Revacept, a therapeutic agent for the prevention and treatment of acute arterial thrombosis, which can lead to heart attack and stroke. It showed specific efficacy in patients and was very well tolerated.
- A Phase II clinical trial in 160 patients with stroke or transient ischaemic attack (TIA) has been completed. It showed beneficial effects in patients treated with 120 milligrams (mg) of Revacept.
- Another Phase II clinical trial investigated Revacept in 332 patients with stable coronary artery disease (ISAR-PLASTER). This study by the German Centre for Cardiovascular Research (DZHK) also showed the very good tolerability of Revacept. In particular, Revacept did not lead to increased bleeding despite additional platelet inhibition on top of maximum thrombocyte inhibition by conventional standard therapy.
- Successor products derived from Revacept combine Revacept in a single molecule with additional functions. These products are also being developed into therapeutics together with academic partners.
- An antibody therapeuticis intended to protect against platelet activation and, in the further course of the disease, also against stroke and heart attack. It is a human antibody fragment (Fab), which was jointly developed with Morphosys AG and is directed against surface receptors (GPVI) on blood platelets. The abbreviation Fab stands for the term “fragment antigen binding” and refers to a different site in the antibody than the “fragment cristallizable” (Fc), which is also important in this context. In laboratory tests, the antibody showed very high specificity and affinity, which were higher than all previously available GPVI antibodies. Efficacy and safety were very convincing in animal experiments.
- Cyclic peptides
for the therapy of thyroid diseases and their complications in the heart and eye.
Stroke and heart attack are the most feared complications of pathological changes in the arteries, atherosclerosis. In these cases, blood platelets (thrombocytes) first attach themselves to the damaged vessel wall. They are activated and attract further platelets, sometimes in very large numbers. In this way a clot, a thrombus, forms inside the blood vessel. This can become so large that it directly seals the blood vessel. Some parts of the blood clot can come loose, float away with the bloodstream and close off smaller blood vessels. This means that the area behind the blood vessel is no longer supplied with blood. This is particularly dangerous in the brain and heart – that is where a stroke or heart attack can happen.
A crucial factor in this process is the attachment of the blood platelets to the wall of the blood vessels. The platelets use different receptors to recognise damage in the blood vessels and attach themselves to them. The most important of these receptors is glycoprotein VI, which is called GPVI and is located in the membrane of the platelets. A large part of the protein hangs in the bloodstream and is water-soluble. It contains the area where it attaches to the wall of the blood vessel.
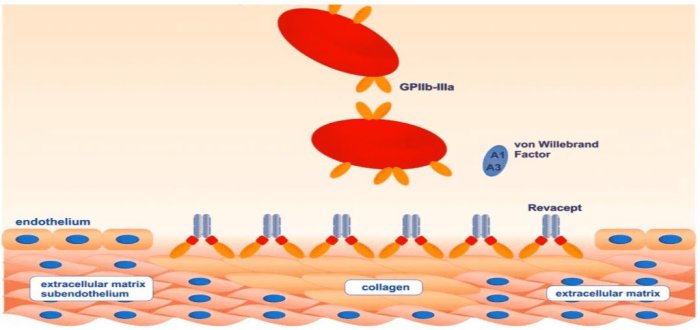
Revacept is a synthetic protein that contains the soluble part of GPVI in one of its two halves, while the other half is formed by the so-called Fc-part of antibodies. There are already many pharmaceuticals containing Fc-fusion proteins. However, Revacept is the first product of its kind to be used in stroke and heart attack.
With its GPVI part, Revacept binds to damage in arteries, thus covering them and forming a kind of vascular patch. This prevents the formation of thrombi in the arteries. However, unlike all other drugs used to treat stroke and heart attack, Revacept does not increase the risk of bleeding. The general haemostasis remains unaffected – and this is the decisive advantage of Revacept.
Revacept has proven to be very effective in laboratory tests with platelets and in animal experiments. In a Phase I clinical trial with volunteers, it was shown to be very well tolerated at all dosages. It induced a specific and dose-dependent inhibition of aggregation (clumping of platelets) in the blood of the volunteers without any relevant side effects. In particular, general haemostasis was not affected: The bleeding time was not prolonged by Revacept and there were no bleeding complications and no reduction in platelet count (thrombopenia).
The first multi-centre Phase II clinical trial (registered under NCT01645306) in 158 patients showed beneficial effects of Revacept in patients with carotid stenosis. The patients had undergone intervention (surgery or catheter treatment) after minor strokes or transient ischaemic attacks (TIA, a preform of stroke). They were given Revacept before the intervention to prevent complications caused by thrombi, which can cause small strokes during or after the intervention. The protocol of the study has been published (Gröschel et al Thrombosis Heamostasis Open 2020).
Magnetic resonance imaging (DWI-MRI) showed that Revacept significantly reduced the number of new brain infarctions associated with the intervention: In the group treated with 120 milligrams (mg) of Revacept, these infarctions were reduced by 46 percent compared to placebo; in the group treated with 40 mg of Revacept, the reduction was still 10 percent. The patients had an overall clinical benefit with significantly reduced combined endpoints of bleeding and ischaemic complications (“net clinical benefit”). The study is published in Stroke (Uphaus et al, Stroke. 2022;53:00–00. DOI: 10.1161/STROKEAHA.121.037006)
The second study was initiated and led by clinical researchers of the German Centre for Cardiovascular Research (DZHK). This so-called “ISAR-PLASTER” study with 330 patients with stable coronary heart disease was conducted by the teams of Prof. Dr. Adnan Kastrati from the German Heart Centre Munich and Prof. Dr. Steffen Massberg from the Großhadern Clinic of the University of Munich together with medical doctors from other large hospitals in Germany. The study is registered under NCT 03315285 and Eudra-CT 2015-000686). Its protocol is published (Schüpke et al, Thrombosis + Haemostasis 2019; 119:1539-1545).
The data proof that Revacept did not increase bleeding complications or other safety issues. The pharmacodynamic proof of efficacy could be obtained in the blood of the patients in aggregation measurements: despite already maximum conventional therapy Revacept additionally inhibited platelet aggregation specifically. However, the primary endpoint of death or myocardial injury was not reached, possibly because technical problems during stenting such as side branch occlusion cannot be addressed by the local effect of Revacept. The study is published in JAMA Cardiology (Mayer et al JAMA Cardiol. doi:10.1001/jamacardio.2021.0475).
The current status of the development of antiplatelet drugs was summarised in a review in 2019 (Arjun Majithia and Deepak Bhatt, Arterioscler Thromb Vasc Biol. 2019; 39:546-557). In addition to the platelet inhibitors already available in clinical routine, the new developments highlight the advantages of Revacept. This independent review underlines the unique properties of Revacept as a specific thrombosis inhibitor without increased risk of bleeding.
Revacept has been developed together with companion diagnostics to provide early and tailored treatment for patients at high risk of arterial thrombosis. The diagnostics uses the fact that soluble GPVI (sGPVI) is released as an early biomarker of platelet activation. In patients with high sGPVI levels, it is hypothesised that the administration of Revacept can specifically prevent the occurrence of thrombosis without affecting or even reducing bleedings as part of a personalised therapy.
Currently Revacept is being prepared to get phase III ready: We have established large scale production in the fed batch process together with Bibitec/Nordmark. The application as an investigational new drug (IND) at the Federal Drug Agency (FDA) is being prepared to get approval for a phase III study in the United States.
Further developments are already on the horizon. For example, successor products to Revacept could combine its positive properties with additional functions and, for example, dissolve existing vascular constrictions, so-called plaques. Such fusion proteins derived from GPVI-Fc with additional effector functions are currently in preclinical development at advanceCOR.
For example, GPVI-fusion proteins were produced with CD39, an enzyme that inhibits local adenosine diphosphate (ADP) accumulation. In laboratory tests, GPVI-CD39 increases the anti-thrombotic effect compared to pure GPVI inhibition. This has been shown, for example, in experiments in which blood was drained from the carotid artery of patients via damaged blood vessel segments. With GPVI-CD39, a potential successor to Revacept is already in the pipeline.